Anti-doping in rugby union: concussion and “compelling justification”

1. INTRODUCTION
The WADA Code (the “Code”) provides that an athlete will commit an Anti-Doping Rule Violation (an “ADRV”) by “refusing or failing to submit to Sample collection without compelling justification after notification by a duly authorized Person” (emphasis added). This provision is incorporated into the World Rugby Anti-Doping Rules, and thus applies across the sport of rugby union.
If an athlete is found not to have a compelling justification they will face a four-year ban, unless they can establish that their failure to submit was not intentional, in which case they will be banned for two years. If it is held that the ADRV was committed intentionally, but that exceptional circumstances exist, the ban may be reduced to between two and four years, depending upon the athlete’s degree of fault. Thus, a (deemed) refusal or failure to submit to sample collection will typically result in a very significant (and possibly career ending) ban.
The rule is intended to ensure that athletes provide a sample when requested to do so. That is important, not only to ensure that athletes who are deliberately doping cannot avoid being tested, but also to ensure wider compliance with anti-doping testing.
However, the rule is not absolute, and instead recognises that there may be a compelling justification why an athlete failed or refused to provide a sample. Notably, the Code does not provide any guidance as to what would, and would not, amount to a compelling justification.
This article considers whether suffering a concussion during a rugby match (or, indeed, whilst playing any sport) should be regarded as a compelling justification, or should otherwise exempt a player from having to submit to sample collection.
2. CONCUSSION
Concussion is a type of Traumatic Brain Injury, often referred to as a mild Traumatic Brain Injury.
The issue of concussion in sport has been well-documented and is of particular concern in rugby union owing to the sport’s high concussion rate. In the RFU’s annual Professional Rugby Injury Surveillance Project, concussion has been the most reported match injury for nine consecutive seasons to 2019/20, and its prevalence in the game has seen it described as an epidemic.
3. CASE STUDY
The authors are aware of one case in which an athlete (“Athlete X”) declined to provide an anti-doping sample having suffered a concussion.
Athlete X was knocked out during a match and remained unconscious for a significant time, receiving on-field treatment before being carried from the pitch. Once off the pitch their cervical spine was “cleared” (i.e. it was established that they had not suffered an injury to their cervical spine), and they were then assessed by the team doctor. The doctor concluded that they did not need to attend hospital, but that they had suffered a concussion.
Whilst still on the spinal board, Athlete X was approached by a Doping Control Officer (the “DCO”) asking them to provide a sample. Athlete X declined, explaining that they did not feel well enough to do so. Some discussion then followed, with Athlete X ultimately recording on the Doping Control Form that they were not providing a sample due to the concussion, and due to feeling unwell.
As a result, Athlete X was subjected to an investigation and provisionally suspended on the basis that they had potentially refused or failed to submit to doping control without compelling justification.
Ultimately, Athlete X was not charged, but this was not before the anti-doping authorities had interviewed them, interviewed other witnesses, and obtained an expert opinion from a neurologist.
Thus, in that case, it was (presumably) accepted that Athlete X had a compelling justification for failing or refusing to submit to sample collection. However, there is no clear guidance as to whether this will always be the case when a player has suffered a concussion.
4. JURISPRUDENCE
What can be said on the basis of the publicly available jurisprudence, is that tribunals have tended to give a relatively restrictive interpretation to “compelling justification”, albeit none of the relevant cases concerned head injuries.
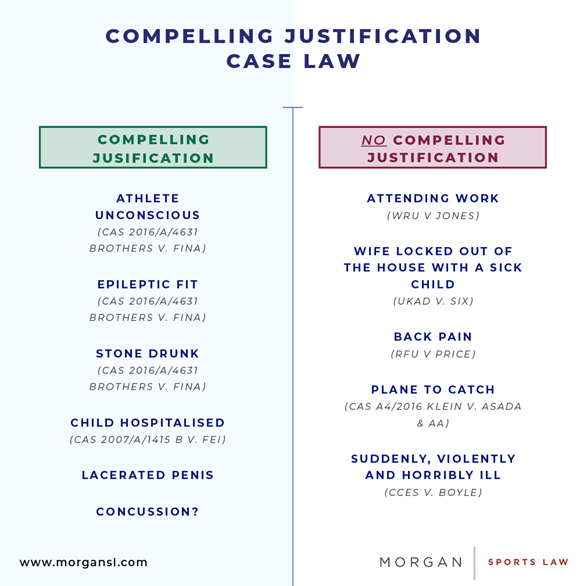
In Jones v. WRU, it was held (by a majority) that a semi-professional rugby player who had to leave urgently for work after being unable to pass urine for some time, did not have a compelling justification for refusing to provide a sample. It held that a reason must be “exceptional, indeed, unavoidable” to amount to a compelling justification.
In CCES v. Boyle, it was held that an athlete being taken “suddenly, violently and horribly ill” would not amount to compelling justification. Somewhat similarly, in UKAD v. Six it was held that a cyclist who had declined to provide a sample because he had just learned that his wife was locked out of the house with their ill son, such that he needed to return home immediately, did not have a compelling justification.
Finally, anxiety and being required to leave for the airport (so as to not miss a flight) have been deemed not to be sufficiently compelling reasons to justify failing to provide a sample.
Nonetheless, tribunals have made clear that there will be circumstances (even absent a head injury) in which athletes will be deemed to have a compelling justification. For example, in CAS 2007/A/1415 B v. FEI it was held (at para. 33) that an athlete’s child being hospitalised would amount to a compelling justification.
In addition, the authors are aware of a case in which an athlete (“Athlete Y”) declined to provide a sample owing to a 4-5cm cut on his penis. Even after being shown the injury, the DCO insisted to Athlete Y that he must provide a sample and that refusing to do so would be an ADRV. Fortunately, the club doctor intervened and explained that Athlete Y needed to go to hospital urgently. No charges were ultimately brought against Athlete Y, as it was (presumably) accepted that there was a compelling justification for his refusal.
As to statements of principle, in CAS 2016/A/4631 Brothers v. FINA, the panel held that:
…If it remains “physically, hygienically and morally possible”, for the sample to be provided, despite objections by the athlete, the refusal to submit to the test cannot be deemed to have been compellingly justified.
Obviously, this would not be the case if the athlete were to faint unconscious on the floor upon seeing the DCO’s needle, or if he were stone drunk or would experience an epileptic fit at the time of the test. Even a refusal to submit to the test because the athlete must rush his expectant wife to hospital might qualify as a “compelling justification.”
Examples of this kind in which it is established that an athlete is deprived of his rationality and cognitive senses will, in most cases, be sufficient to ground the excuse of “compelling justification”. These situations present physical and moral hindrances to going ahead with the test.
(Emphasis added)
Thus, in Brothers the panel stated that where it has been established that an athlete was deprived of their rationality and cognitive senses, that will, “in most cases”, amount to a compelling justification.
That guidance is of some assistance but, even ignoring the unhelpfully vague caveat of “in most cases”, it remains unclear whether an athlete that has been concussed will always be considered to have been deprived of their rationality and cognitive senses.
5. CONCUSSION AS A COMPELLING JUSTIFICATION (OR OTHERWISE AS A DEFENCE)
Notwithstanding the largely restrictive approach previously taken by tribunals (albeit not in the context of head injuries), it is the authors’ view that concussion must be considered a compelling justification, or otherwise to be a total defence to a charge of failing or refusing to submit to sample collection.
Whilst a concussed (but conscious) player may physically be able to provide a sample, their cognitive function will be impaired such that they may not be able to understand and/or retain information provided to them by the DCO, or to form rational judgements. Moreover, in such a situation, it will be impossible for a DCO to accurately assess a player’s level of rationality and cognitive function.

In such circumstances, it cannot properly be said that sample collection is “morally possible”. Indeed, such an individual may be said to lack legal capacity, such that they could not lawfully consent to providing a sample for analysis. Crucially, this is not the same as a player simply being ‘ill’ – when concussed, players do not just feel unwell, their brains are fundamentally compromised.
Further or alternatively, such an individual cannot properly be notified of the requirement to submit to sample collection (given their altered neurological state) and thus no ADRV would be committed on that basis (prior “notification by a duly authorized person” being a condition precedent to any ADRV).
Of course, some might suggest that such an approach would open the door for unscrupulous players and/or team doctors to avoid doping control by feigning concussions. However, any such concern is overstated. First, such conduct would amount to Tampering under the Code – an ADRV carrying a likely four-year ban – whilst a doctor’s involvement in such a ruse would, if uncovered, result in severe professional consequences (in addition to anti-doping liability for the doctor). Second, such underhand behaviour could be guarded against by requiring a doctor to sign off on the player’s concussion diagnosis and thus to declare them unfit to provide a sample. At elite level, this responsibility could be given to the independent matchday doctor, to reduce the risk of unscrupulous teams influencing their medics.
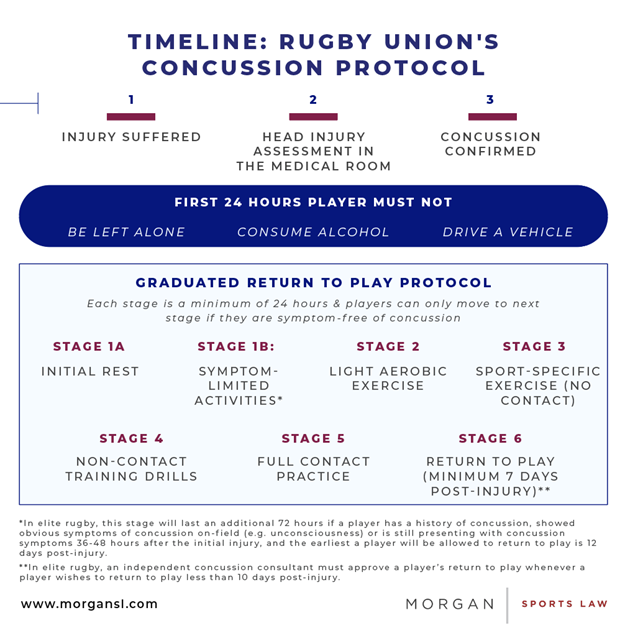
Further, rugby’s Graduated Return to Play Protocol (the “GRTP”) mandates that concussed players must pass a series of tests, over a minimum of six days, in order to be able to return to play, and this process will ordinarily be carefully documented. In some cases, this will inevitably rule a player out of the next match and, in all cases, this will require the player to take a reduced role in training. Moreover, in the elite game, team doctors are now required to seek the opinion of an Independent Concussion Consultant (“ICC”) in respect of any concussed player who is expected to return to play within 10 days. A player feigning a concussion to avoid doping control would therefore also have to comply (or feign compliance) with the GRTP and ICC processes to avoid suspicion, making such a deceit less likely (particularly given the risk of missing matches) and more readily detectable.
In any event, the protection of players’ fundamental rights and welfare must surely trump the risk that some might attempt to abuse such a system. Indeed, in boxing (at least in the UK), the authors understand that athletes will only be required to provide a sample, following a fight, if they are first declared fit to do so by the event doctor.
It is therefore the authors’ view that a rugby player who is removed from the pitch due to concussion, should be entitled to decline to submit to doping control, without consequence. However, to safeguard the doping control process, the player’s (diagnosed or suspected) concussion removal should be documented by a team official, and a documented medical assessment carried out thereafter.
6. CONCLUSIONS
The idea of a concussed player being subjected to anti-doping tests is a troubling one.
The lack of certainty surrounding such a player’s anti-doping obligations and the consequences that may flow from their refusal or failure to provide a sample puts players (and also the medics responsible for their care) in a difficult position. Moreover, given their brain injury, a concussed player will likely be unable to properly comprehend the situation or the potential consequences of a refusal to provide a sample.
It might be suggested that a solution to this problem would be for DCOs to wait until the player has recovered from their injury (shadowing the player throughout), and then to collect the sample. Yet complete recovery from concussion may take days, if not weeks – rendering such an option entirely impractical – whilst it would also result in DCOs having to make (medical) judgements about a player’s capacity, which is part of the original problem. Indeed, a better solution would be for the DCO to simply test another player from the team.
The authors therefore call upon World Rugby, following consultation with WADA, to:
- i) implement guidance to make clear that players who have been diagnosed by a doctor as having suffered a concussion shall not be required to submit to doping control for at least the first 24 hours following the injury; and
- ii) ensure that all DCOs tasked with collecting samples in rugby union receive adequate concussion awareness training.
These actions would give due recognition to the seriousness of concussion as a brain injury and would better respect the rights and welfare of players.
Authored by
Tom Seamer
Barrister
Ben Cisneros
Associate
Footnote
1. See Article 2.3 of the Code
2. See World Rugby Regulation 21.2.3
3. See Article 10.3.1 of the Code
4. Albeit it should be noted that tribunals have applied the No Fault (e.g. UKAD v. Bailey (NADP Tribunal, 8 December 2017) at www.rb.gy/ig7xca) and No Significant Fault (e.g. CAS 2016/A/4631 Brothers v. FINA (www.rb.gy/ybmgib)) provisions of the Code to eliminate or reduce the otherwise applicable sanction. Further, in CAS A4/2016 Klein v. ASADA & AA (www.rb.gy/egtvna), the CAS applied the principle of proportionality to reduce the otherwise applicable sanction.
5. McCrory P, Meeuwisse W, Dvorak J, et al., Consensus statement on concussion in sport—the 5th international conference on concussion in sport held in Berlin, October 2016, BJSM 2017; 51: 838-847 (at XXX).
6. See, for example, ‘Head in the Game: Concussion & Sport’ (at www.rb.gy/zorres) and the UK Parliamentary DCMS Committee report on ‘Concussion in sport’ (at www.rb.gy/peuysb).
7. See the England Professional Rugby Injury Surveillance Project, Season Report 2019-20 (at www.rb.gy/4dsckg)
8. Marshall SW and Spencer RJ, Concussion in Rugby: The Hidden Epidemic, J Athl Train. 2001; 36(3): 334-338 (at www.rb.gy/vctpzv).
9. The authors do not know for certain the grounds on which it was decided not to charge Athlete X. However, it seems most likely that it was accepted that Athlete X had a compelling justification for not providing a sample. Another possibility would be that it was concluded that Athlete X could not have been properly “notified” of their need to submit to sample collection, given their condition, such that no ADRV could have been committed (as to which see Section 5 below). In either event, no charge would have been brought due to Athlete X’s concussion.
10. The player’s father, for whom the player worked, gave evidence that if he and his son had not attended at the relevant work site at the appropriate time, there was every possibility that the material being delivered to site would have been driven off site and dumped, at a cost of approximately £900 to the business.
11. See WRU v. Jones (NADP Appeal Tribunal, 9 June 2010) at para. 57 (see www.rb.gy/aqxgbx)
12. CCES v. Boyle (SDRCC, 31 May 2007) at para. 53 (see www.rb.gy/9yu1im)
13. UKAD v. Six (NADP Tribunal, 25 October 2012) at www.rb.gy/tolh6j. Cf. CAS 2007/A/1415 B v. FEI (at para. 33) where it was held that a child being hospitalised would amount to a compelling justification (see www.rb.gy/hoth2l)
14. CAS 2016/A/4631 Brothers v. FINA (www.rb.gy/ybmgib)
15. CAS A4/2016 Klein v. ASADA & AA (www.rb.gy/egtvna)
16. Nonetheless, the DCO’s view remained that Athlete Y had committed an ADRV and it took the Anti-Doping Organisation in question four months to determine that Athlete Y had no case to answer.
17. Noting that, contrary to Athlete X, Athlete Y would not appear to have had a defence based on the notification requirement (as it seems unlikely, albeit perhaps not impossible, that Athlete Y’s mental faculties would have been affected by the injury).
18. See, for example: McInnes K, Friesen CL, et al, Mild Traumatic Brain Injury (mTBI) and chronic cognitive impairment: A scoping review, PLoS One. 2017; 12(4): e0174847 (at www.rb.gy/2fbtba); Rabinowitz AR and Levin HS, Cognitive sequelae of traumatic brain injury, Psychiatr Clin North Am. 2014;37(1):1-11 (at www.rb.gy/iqle5r); and Covassin T and Elbin RJ, The cognitive effects and decrements following concussion, Open Access J Sports Med. 2010; 1: 55-61 (at www.rb.gy/9lc5tf).
19. See, for example, Turner M, Maddocks D, Hassan M, et al, Consent, capacity and compliance in concussion management: cave ergo medicus (let the doctor beware), British Journal of Sports Medicine 2021; 55: 539-544 at 541-533 (at www.rb.gy/wvsb4w); and NHS, Consent to treatment – Assessing capacity (at www.rb.gy/k0v4b8). In the event that an individual lacks capacity to consent, tests and/or treatment may only be performed if they are in the individual’s best interests (see, for example, Re T [1992] EWCA Civ 18); and NHS, Consent to treatment – Overview (at www.rb.gy/osoowq).
20. For example, as a result of the ‘bloodgate’ scandal, physiotherapist Steph Brennan was struck off by the Health Professions Council (though subsequently won a High Court appeal) and doctor Wendy Chapman was suspended and subsequently given a warning by the GMC. See: https://www.irishtimes.com/sport/rugby/sporting-controversies-bloodgate-and-the-afternoon-that-forever-stained-harlequins-1.4244612
21. C.f. ‘Bloodgate’ (see: https://www.irishtimes.com/sport/rugby/sporting-controversies-bloodgate-and-the-afternoon-that-forever-stained-harlequins-1.4244612)
22. See: https://www.world.rugby/news/653076/independent-concussion-consultants-to-be-introduced-to-support-graduated-return-to-play-process-in-elite-rugby
23. See: https://www.nhs.uk/conditions/head-injury-and-concussion/